


Long Covid Doubt
How Doubting People’s Long Covid Symptoms Causes Patients Harm
Last week in the Long Hauler COVID-19 support group, an anonymous member posted something that I’ve heard several times from Long Haulers. It was a guttural plea to be believed. This post linked the consistent disbelief that they experience in all aspects of their lives, from doctors, government, family, friends, and neighbors to a private pain of feeling forgotten. People are exhausted by having to prove again and again that their symptoms are real and that they deserve to be heard.
I can't explain the trauma. It's horrifying when it hits me. Too much. And it hits me harder when my brain's awake and has the capacity to conclude this really is happening. What a vicious cycle. It's like my brain is half asleep most of the time due to sickness or sensory overload, I guess - not really comprehending how horrifying it is to feel your heart fail to maintain it's steady beat or to suddenly lose your breath as your vision narrows.. or feel the periodic and bizarre shocks among countless unexplainable symptoms of an out-of-control nervous system.
At this point, normal days can't be trusted. People seem to have a mocking and condemning, yet quiet connotation when they tell me, whether my own mother or medical doctors, that these symptoms are all in my mind…
Me fighting to make them understand:
"But they're real symptoms."
Them with a quiet, patronizing voice:
"I know they're real.. to you, Jerry"
How devastating and cruel. Kind of like Texas Chainsaw Massacre when the girl is running for her life to find herself in the quiet atmosphere of the eerily soft-spoken ladies trying to lull her to death. The contrast is torture. That's what it feels like to me.
I've passed out on hospital beds, fighting for air with an erratic heart rate, to the sound of alarms on the monitor to be told there's nothing wrong. I've made appointments by the skin of my teeth with my head swelling with pressure, my vision crossed and faded, my legs weak, and my voice slow and slurred, just to fall into the same old cliche of irritated doctors dealing with a mental patient.
What is this? Did I die already?
I literally have to fight with thoughts like that because my frazzled mind scours the realm of bizarre likelihoods to find something that makes sense and "you're just anxious" does not register as a plausible conclusion. "You're just depressed", mentally, has been overwhelming proof that I've slipped through the cracks of medical explanation and that I'd do just as well to shut up and die however bizarre and debilitating these symptoms might be.

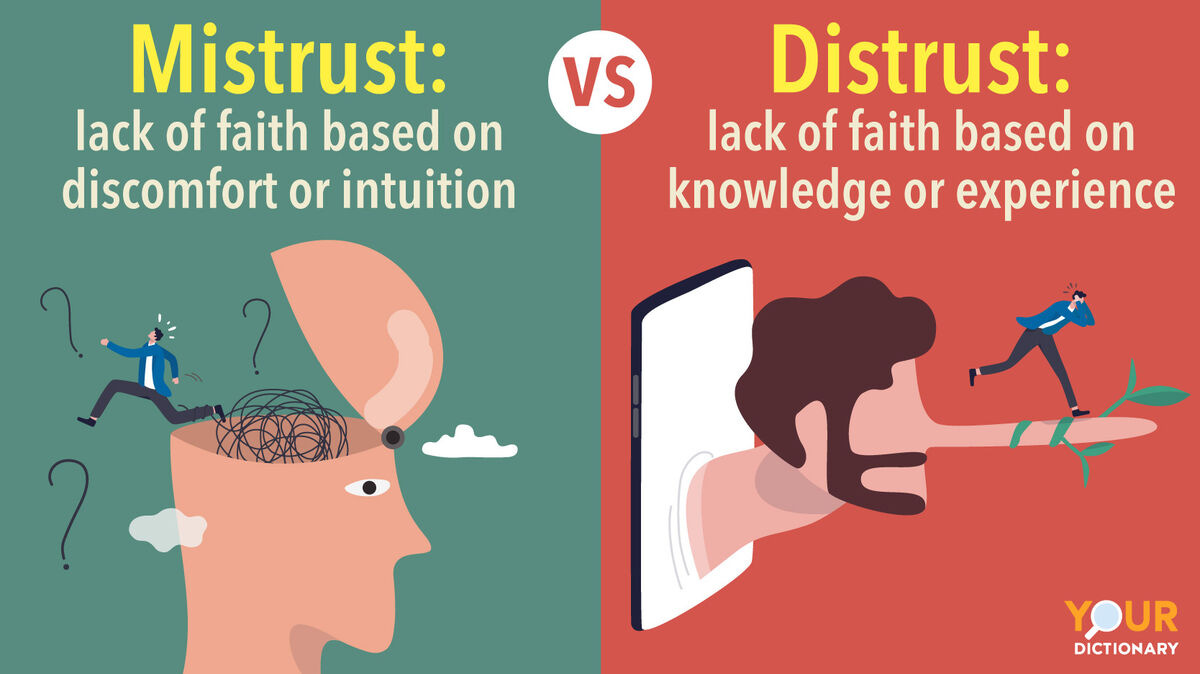
Mistrust in medicine and the government is a frequent topic of conversation in my discussions with people experiencing Long Covid and other contested illnesses. In her beautiful book, Invisible Kingdom, Megan O’Rourke wrote, “In the middle of the night, when I woke in the dark with my heart pounding, what really terrified me was the conviction that my doctors did not believe me, and so I would never have partners in my search for answers—and treatments. How could I get better if no one thought I was sick?” (pp. 104). While there is a longstanding mistrust of American medicine among Black Americans, mistrust of science in general has become a powerful part of American culture and affected clinical care over the past three decades.
A great deal of this mistrust is based in experience. I spoke to a nurse practitioner in Chicago who said they were not encouraged to diagnose Long Covid. She looked me in the eye and said, “The symptoms are real but I’m not sure Long Covid is real.” This is a common complaint clinicians dismissed patients who presented with Long Covid symptoms, often saying it wasn’t real, or it’s all in your head. This deference is long experienced by people living with contested and chronic illness.
Jen Fricas, a professor of nursing and public health who has lived with ME/CFS for years, put it most clearly. She said, “I think investigating the origin of mistrust is important when we're trying to differentiate these things.” She teaches nurse practitioners about vaccine hesitancy and anti-vaccination movements in part to explain why patients push back or avoid medicine altogether. She explained very pointedly what most of my interlocutors have been saying:
“One of my big pet peeves is when people talk about mistrust. They think, Black people don't trust the system as if it's some problem with Black people not being able to trust as opposed to a problem with the system being abusive. And so I think that thinking about where does the mistrust come from is an important differentiation.”
While medical racism is a deep-seated in American culture, I hadn’t connected the dots yet about which systemic issues are driving the mistrust of people living with contested illnesses like Long Covid.
“For mistrust among people who have experienced medical trauma and gas lighting, it comes from their lived experiences of having illnesses, conditions, things wrong with their body, and being told by people in authority that they actually don't. So you know, the medical community completely disregards their testimony.”
When I followed up with her about this quote, Dr. Fricas told me that what she really was focusing on was the difference between testimonial injustice and hermeneutical injustice. She said this video conveys these concepts, although she was most focused testimonial injustice. This concept of testimonial justice addresses the challenge that one’s account of one’s life is disbelieved or not given acknowledgement or weight in a conversation. She says hermeneutical injustice is also common, especially with long COVID. In this case, there is injustice in having an individual’s social experience obscured from the collective identity owing to broader prejudice against people living with contested illnesses. She mentioned, “Since it is new, even the people who are experiencing it do not have a shared language or terms to be able to accurately describe what they are going through. In this way, it is hard for them to explain with “authority” their experience because accurate or apt terms are not developed or well-known yet.”
Dr. Frica’s comments reminded me about a different situation when individuals felt dismissed by medicine, which has caused societal harm as well as individual harm. I found that the more medical practitioners doubt the validity of what people are saying about their concerns, experiences, or symptoms related to Long Covid, the more doubt is sowed in medicine’s ability to improve health and wellbeing. Now stay with me, because I am going to make a point that might not seem entirely clear at first. I think there are similarities in the experience of people living with contested illness and those I interviewed who were vaccine hesitant in my study of Okoboji, a small rural town in northwest Iowa, which was the subject of my recent ethnography, Unmasked: COVID, Community, and the Case of Okoboji. (I have modified the following three paragraphs from my book—please refer to chapter 10 of Unmasked for a much deeper discussion of vaccine hesitancy—but you will note the resemblances in this way of thinking about mistrust in relation to vaccines and contested illness.)
In her book Stuck: How Vaccine Rumors Start—and Why They Don’t Go Away, Heidi Larson argues that the greatest challenge is that it took so long for those working in health and immunization to realize how deeply rooted the beliefs of the doubting public had become. Larson argues “some of these views have hardened to the point of no return, further nursed by the broader societal and political polarization in which the vaccine debates are situated” (p24). I argued in Unmasked that this polarization was driving the trend that anti-mask groups became bound to anti-vax groups, contending that both are arguments for personal freedoms.
“So where did that come from?” I asked Minnie, a family friend who I had known for several years and resided in the community. “They honestly think that that’s the right thing to do,” Minnie explained. These women fit the anti-vax mold Reich described. She said, “Notably, these women who are racially, educationally, or socioeconomically privileged in some contexts are diminished in others” and “create, promote, and share information to define themselves as experts on their children and on vaccines. These claims of expertise serve to validate their choices and increase their claims to social capital in their networks” (112-116).
This concept of testimonial justice makes sense here: where people feel that their life stories are disbelieved or not given weight in conversation—at least in biomedical spaces. This causes friction within conversations with biomedical practitioners but promotes solidarity within the social networks they foster. Many people living with Long Covid believe that medicine is harmful when biomedical practitioners do not take their symptoms seriously and believe this dismissal is causing them and others harm. Clinical doubt of people’s lived experiences, or the collective biomedical perception that Long Covid is imagined or unreal, then, not only diminishes people’s lived experiences but also sows deep mistrust.
Ja’Mia Hewitt has lived with Pots since she was eight and her experience living with Pots was one reason she went into nursing. This experience has been invaluable as she’s navigated her Long Covid. She told me, “If I weren’t a nurse, I don’t even know where I’d be right now. That’s why I’m so concerned about people who don’t have a healthcare background. They don’t know what their rights are. That they can get a second opinion. That they can go out of state to get the care they need. What does it look like? Long wait times, bad bedside manner. It’s exhausting.”

Likely anti-vax promotors and people living with Long COVID are more likely to disagree than agree on many things, such as what clinical medicine and public health can or should do to prevent infections. (In other words, most people with Long Covid are advocates of vaccination.) However, there are some important things we can learn from the resistance movements. First, there is allegiance in community-building. Second, there are similar beliefs and shared experiences that drive mistrust in and avoidance of clinical medicine. Third, there are collective solutions built together in online communities. These needs for patient activism reveal the cracks in the medical system. However, while one community rejects medical advice, the other seeks for more answers, treatments, and recognition.
The differences in illness experiences matter. Ja’Mia told me, “Navigating this healthcare system is like pulling teeth. How terrible is it for clinicians to help get diagnoses for patients? For taking seriously for patient care?”
Long Covid, just like ME/CFS, differs in symptoms and severities over time and between people. This is one of the major challenges that makes diagnosis such a difficult sell for clinicians. In fact, this complexity is highlighted on the CDC website describing Long Covid of Post-Covid Sequalae: “Long COVID is not one illness. Your healthcare provider considers a diagnosis of Long COVID based on your health history, including if you had a diagnosis of COVID-19 either by a positive test or by symptoms or exposure, as well as based on a health examination.”
The first reason diagnosis is so difficult is because of the heterogeneity of patient symptoms. Many people struggle to sleep, staying awake all night due to anxiety, restless legs, or numbness. Others struggle with memory, from short term to long term, and there is a variance in what types of memory and confusion people experience. While some people may present with a form of dementia, others struggle with word recall. Many people feel pain in the joints and the muscles and experience migraines or constant headaches. Some people experience night sweats. While some people experience depression, and many clinicians find this a defining feature of ME/CFS and Long Covid, many patients argue that the somatic complaints are primarily viral or social in nature. In part, this determination is working against a common phrase mentioned by clinicians (either directly or indirectly) that Long Covid and/or ME/CFS is imagined or unreal, an inflammation of other real diagnoses and conditions.
However, not all clinicians are deterred by the collection of symptoms people present with Long Covid. Dr. Dahlene Fusco explained that she’s seen too many patients with consistent symptom profiles to think Long Covid is not real. Every single person in the clinic with Dr. Fusco says it’s confusing and they fear that they have something that has become a hot-button issue like Chronic Lyme. There is so much stigma and confusion related to those diagnoses. She tells them, “Don't give yourself a diagnosis or a term. Just tell me and tell your other providers what your symptoms are. It's gonna take providers a long time. [For clinicians who don’t recognized Long Covid], I would encourage people to avoid them because they are not reading the CDC website. But and I think we do need to call out providers who are misinformed.”
The second reason diagnosis is so difficult is the lack of a biomarker, or “silver bullet” for diagnosis. In many cases, debility is a combination of many things, perhaps triggered by one thing (like SARS-CoV-2), with an underlying history of previous infections that have lingered in viral reservoirs, traumas that have irreversibly affected the body, and chronic stressors that may be anything from micro-aggressions to insulin sensitivities. Half of people who experience chronic fatigue and other related symptoms for several months or years have experienced one or more of the following diagnoses: infections, anemia, thyroid dysfunction, diabetes mellitus, and cancer. Yet, clinicians find these data inconclusive to predict what may have triggered complex illnesses like ME/CFS and Long Covid.
The final major issue is that clinicians are overwhelmed, overscheduled, and rushed. The increasing number of patients clinicians must see per day, combined with inadequate access to social services resources, often causes clinicians to feel overwhelmed. Some of this overwhelm may be misdirected—especially in emergency departments where “chronic utilizers” or “frequent flyers” constantly seek urgent care. Like other marginalized communities, chronic care-seekers do so because they don’t have the funds or sustainability to engage in routine medical care, or they delay care when they are doubted. When people are told their Long Covid is not real, or their symptoms are imagined (all in your head), people stop seeking care. Then, when things go from bad to worse, people seek acute care. This is not cost effective from the purview of a hospital administrator or patient. It’s preventable.
As Dr. Wes Ely told me, “We need to start listening to people, even though we don't have the test or the diagnosis or the therapy. We have to accompany them. We have to. We have to dive into their chaos and provide uplifting and healing by being present with them.”